Phase 01
Animal Model
40patients
Ref. 10Cardiac Diaphragm Support
VisONE™ Synchronized Diaphragmatic Stimulation addresses the therapeutic gap for HFrEF patients who remain symptomatic despite GDMT — without placing any hardware in the heart.

Many patients with HFrEF remain symptomatic and at high risk despite optimized GDMT, and most — those with a narrow QRS — are not candidates for CRT. VisONE SDS is designed to address this gap with a non-cardiothoracic, minimally invasive approach.1-3
Demonstrated Significant Improvements In Heart Failure Symptoms4-7
Precisely timed diaphragmatic stimulation synchronized with the cardiac cycle — reduces intrathoracic pressure, augments cardiac output.4,8
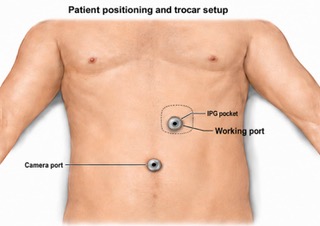
Minimally Invasive Non-Cardiothoracic Laparoscopic Procedure4-7
FDA Breakthrough Device Designation. IDE pivotal trial RECOVER-HF actively enrolling. NCT06552637.
See how VisONE™ delivers precisely timed diaphragmatic stimulation synchronized with the cardiac cycle.
For healthcare professionals. Illustrative purposes only.
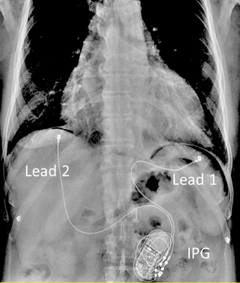
During a minimally invasive laparoscopic procedure two leads are attached to the underside of the diaphragm. The leads provide electrical stimulation to a small section of the diaphragm muscle in synch with the cardiac cycle. The implantable pulse generator is implanted subcutaneously into the abdomen.
Nothing is implanted in the heart.
Minimal scarring, two small incisions in your abdomen to place the device.10
The stimulation is small, patients don't feel it.4,5,10

Active Fixation Lead

Implantable Pulse Generator
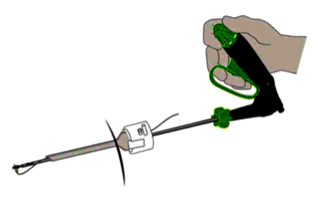
Lead Placement Tool
Clinical development
No Procedure, Therapy Or Device Related MARCE/AEs To Date
Lower is better
Change vs. control
+61 m
p < 0.01
6MWTD (m)
Lower is better
Change vs. control
8 pt improvement
p < 0.05
MLHFQ (au)
Lower is better
Change vs. control
7% improvement
p = ns
LVESV (%)
Lower is better
Change vs. control
3.9% improvement
p = ns
EF (%)
Lower is better
Change vs. control
+1.4 L/min
p < 0.01
LVCO (L/min)
SDS group vs. baseline
* Study not powered for significance.
** Compared to baseline.
IDE Pivotal Trial
Prospective, multi-center, double-blinded, sham controlled randomized safety and efficacy trial. ClinicalTrials.gov NCT06552637
Patient Population